Sound Pollution From Auditory Discomfort to Cardiovascular Mortality
Why Acoustic Design Is a Public Health Imperative
The physical parameters of building acoustics and environmental noise do not merely govern comfort; they act as potent modulators of human physiology [1]. While historical regulations focused almost exclusively on preventing direct, energy-dependent auditory damage, contemporary environmental medicine recognizes a continuous, multi-system pathological spectrum [1]. This spectrum begins with localized sensory discomfort and speech interference, escalates through neuroendocrine and autonomic dysregulation, and ultimately contributes to chronic systemic illnesses and premature mortality [1].
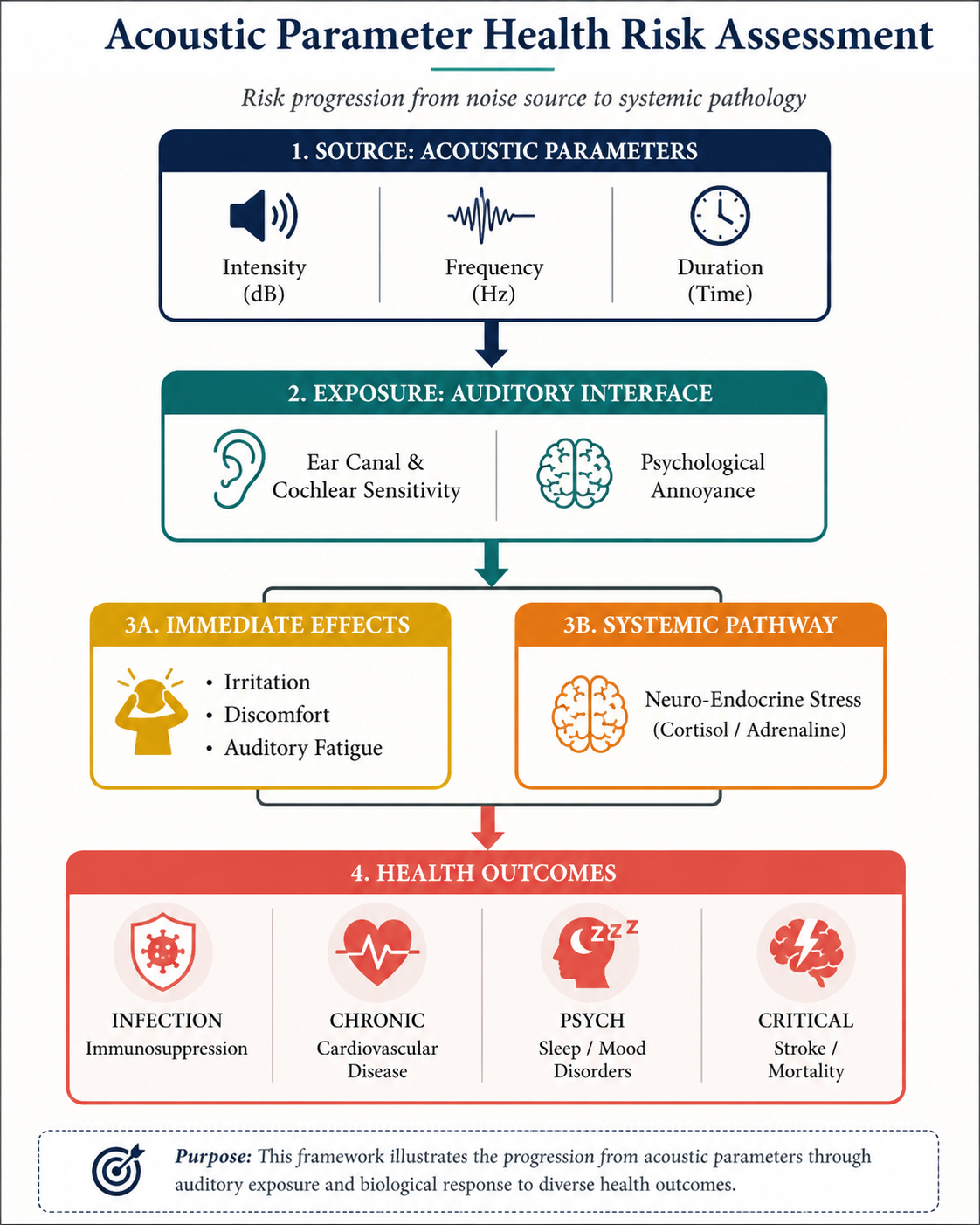
To systematically analyze these human responses, environmental and architectural research maps the relationships between physical building parameters and physiological outcomes [1]. A critical visual and conceptual framework for this analysis is established by the matrix mapping building physics to human health responses [6].
By examining how specific acoustic parameters such as sound level, frequency, duration, absorption, and sound insulation interact with broader environmental conditions such as air pollution concentration, researchers can trace the causal pathways through which physical acoustic parameters translate into chronic illness and death [1].
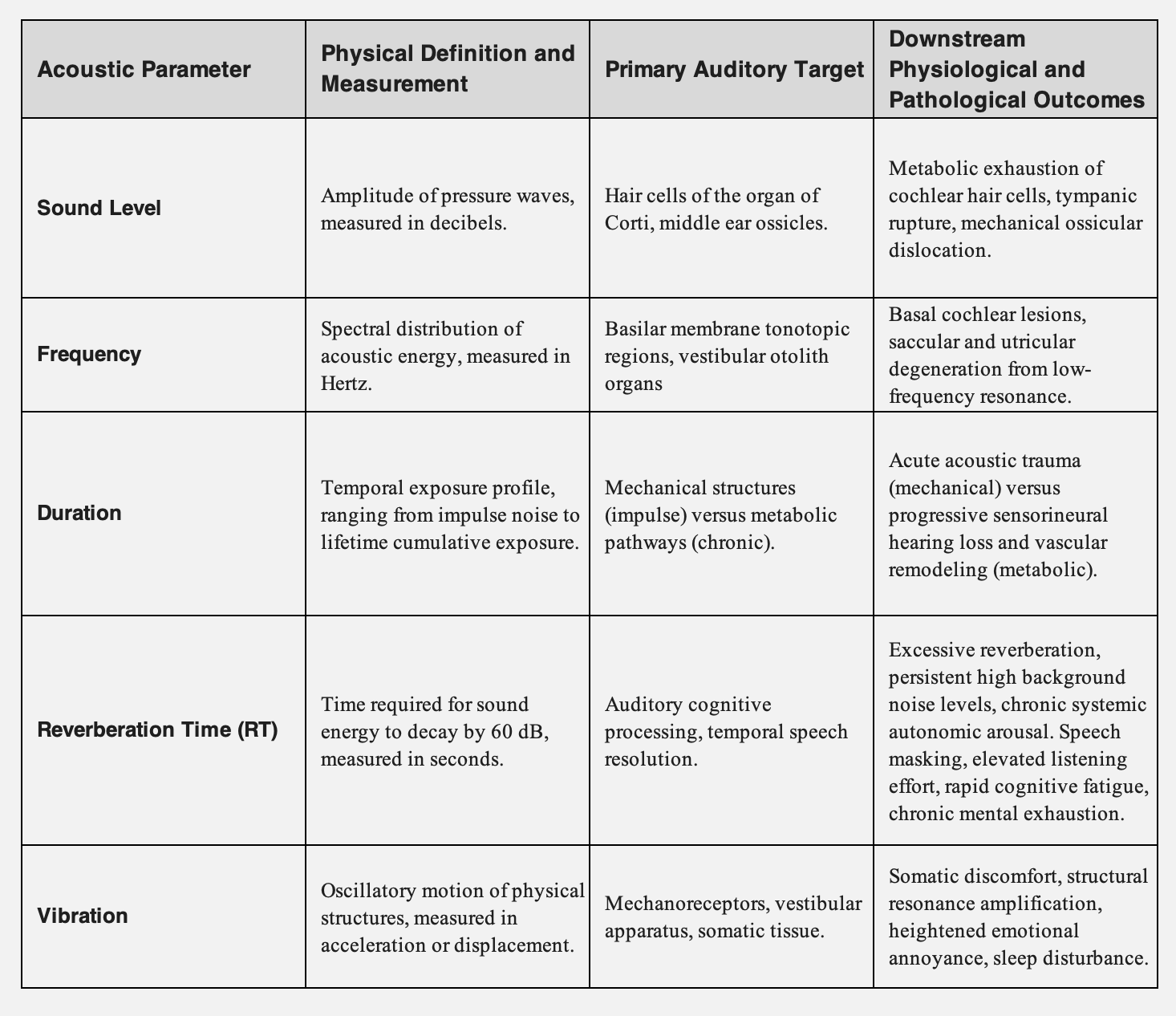
Physical Parameters of Building Acoustics and Human Health
Human responses to the indoor environment are dictated by a matrix of physical parameters within the domain of building physics [1]. These parameters do not operate in isolation; rather, their combinations govern both the energy load on the auditory apparatus and the degree of psychological and physiological stress experienced by occupants [1].
Sound Levels, Frequencies, and Durations
The amplitude or sound level of an acoustic stressor determines whether its impact is primarily mechanical or metabolic[9]. High-decibel exposures are categorized into chronic exposures (such as prolonged occupational noise between 80dBA and 100 dBA and acute impulse exposures such as blasts or gunfire exceeding 140 dB lasting less than 0.2 second [8].
The human ear exhibits frequency-dependent sensitivity, with the highest vulnerability located in the 2kHz to 5kHz range [10]. High-intensity acoustic energy concentrated in this frequency band causes localized lesions on the basilar membrane [9].
In contrast, low-frequency noise typically spanning 0.5 to 200 Hz or lower possesses long wavelengths that easily bypass standard architectural barriers [11]. Low-frequency sound waves travel deep into the inner ear, where they cause mechanical shear stress on both the auditory hair cells and the vestibular otolith organs the saccule and utricle, leading to concurrent balance and hearing deficits [11].
Absorption, Sound Insulation, and Reverberation Time
The physical configuration of indoor spaces dictates the behavior of sound waves.1 Sound insulation parameters determine the attenuation of external noise penetrating the building envelope, while the absorption characteristics of internal boundaries regulate the decay of acoustical energy [1].
When sound insulation is poor, or internal boundaries lack sufficient absorption, spaces suffer from elevated background noise and prolonged reverberation times (RT) [15]. A high RT creates a persistent diffuse sound field where reflected acoustic energy overlaps with direct speech signals [15]. This temporal and spectral smearing masks high-frequency consonants, which are critical for speech intelligibility, thereby increasing the listening effort required by occupants [15].
Structural Vibration and Annoyance
Acoustic energy can couple with building elements to cause structural vibration. These low-frequency physical oscillations are felt directly through somatic tissue and are registered by mechanoreceptors throughout the body [1].
Structural vibration amplifies the subjective degree of annoyance, transforming a physical acoustic parameter into a chronic psychological stressor [1]. This persistent annoyance is not merely a quality-of-life issue; it acts as a primary trigger for the sub-cognitive stress pathways that drive long-term cardiovascular pathology [16].
Interactions with Pollution Sources and Air Concentration
A major advancement in indoor environmental quality (IEQ) research is the recognition that acoustic parameters interact dynamically with air pollution concentration [1]. In poorly ventilated modern buildings, chemical pollutants such as formaldehyde and volatile organic compounds and biological pollutants such as mold spores and dust mite allergens accumulate to high concentrations [1]. These airborne pollutants cause physical irritation, mucosal swelling, and chronic inflammatory changes in the respiratory tract and nasal passages [1].
At the human level, these stress factors interact synergistically [1]. High concentrations of chemical pollutants irritate the upper respiratory mucosa, causing localized inflammation and congestion of the Eustachian tube [1]. This congestion compromises middle ear ventilation, altering the impedance of the tympanic membrane and increasing the vulnerability of the middle ear to acoustic stress [23].
Furthermore, laboratory experiments demonstrate that when humans are exposed to concurrent stressors such as background noise combined with high concentrations of chemical pollutants the central nervous system integrates these inputs, resulting in a heightened perception of both acoustic annoyance and mucosal irritation [7].
The Pathological Hierarchy of Human Acoustic Responses
The human body's response to acoustic parameters operates as a pathological hierarchy [1]. Each stage of this hierarchy corresponds to distinct physical thresholds, cellular mechanisms, and clinical endpoints [1].
Auditory Discomfort: Speech Interference, Annoyance, and Cognitive Overload
At the base of the pathological hierarchy lies auditory discomfort, clinically characterized by localized disturbance, speech interference, and heightened annoyance.1 In learning and working environments, background noise (dB) and reverberation time (second) dictate the severity of this discomfort [15].
When RT in a classroom or office exceeds 0.6 seconds, the diffuse, reverberant speech energy overlaps with the direct voice signal [15]. This creates temporal masking, requiring listeners to exert high cognitive effort to filter out background noise and reconstruct masked phonemes [18].
To compensate for this degraded signal, the brain's prefrontal cortex must recruit working memory resources [18]. This continuous cognitive load limits the mental resources available for high-level tasks like reading comprehension, mathematical reasoning, and spatial memory [19].
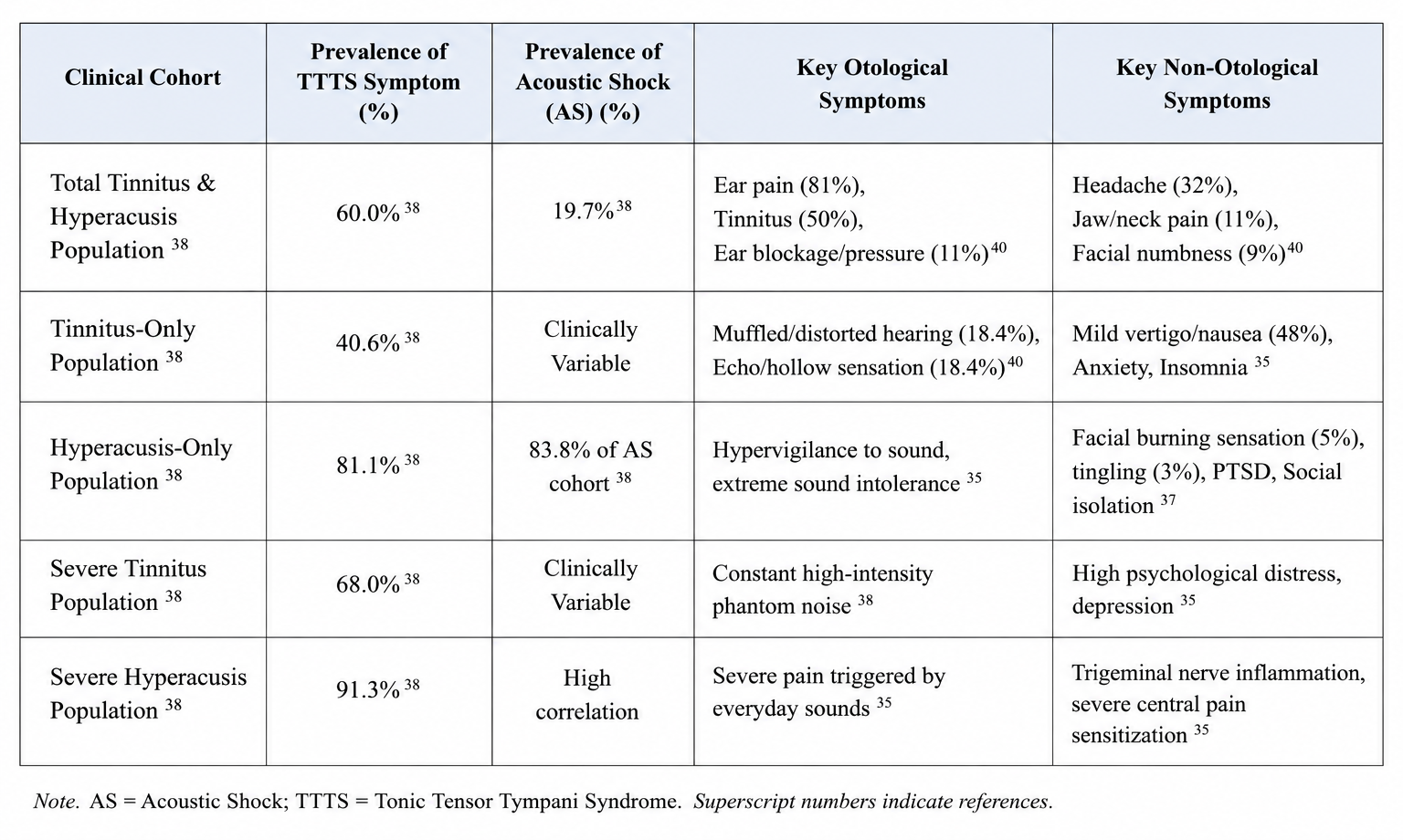
Clinical Cohorts - TTTS Prevalence - Acoustic Shock - Otological Symptoms
In children, whose top-down language processing and auditory pathways are still maturing, the presence of elevated background noise exceeding the recommended standard of 30 dBA significantly hinders learning progress [15]. In adults, teaching or working in rooms with poor acoustics high RT ranging from 0.6 to 1.0 causes early fatigue, sleepiness, loss of motivation, and a statistically significant drop in job satisfaction [17].
Systemic Effects: Tiredness, Sleep Fragmentation, and Vestibular Degradation
When exposure to acoustic parameters is chronic, localized discomfort escalates into systemic physiological consequences, clinically presenting as chronic "tiredness" and autonomic fatigue [1]. This systemic degradation is mediated by the autonomic nervous system (ANS) and the endocrine system [16].
Chronic noise exposure activates the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system (SNS) [28]. The amygdala detects acoustic energy as an environmental threat, bypassing conscious cognitive processing, and triggers the following pathways 16:
● The Sympathetic Pathway: Stimulates the adrenal medulla to release catecholamines, namely epinephrine (adrenaline) and norepinephrine, into the bloodstream within seconds [29]. These hormones bind to cardiovascular (Beta) adrenergic receptors, driving rapid vasoconstriction, elevating heart rate, and increasing blood pressure [28].
● The Endocrine Pathway: Prompts the hypothalamus to release corticotropin-releasing hormone (CRH), driving the anterior pituitary to secrete adrenocorticotropic hormone (ACTH) [29]. ACTH stimulates the adrenal cortex to synthesize and release the glucocorticoid cortisol [29]. Cortisol raises blood glucose levels through gluconeogenesis, alters immune cell distribution, and enhances vascular sensitivity to catecholamine-induced constriction [29].
Under continuous environmental or nocturnal noise exposure, this fight-or-flight response remains active, causing a state of chronic autonomic arousal [31]. Nocturnal transport noise is particularly destructive [2]. Even when noise levels do not fully awaken an individual, exposure to levels exceeding 40 dBA - 45 dBA causes autonomic micro-arousals [2]. These micro-arousals disrupt deep sleep stages, trigger spikes in stress hormones, and prevent the natural nocturnal blood pressure "dipping" process, leaving the cardiovascular system under continuous strain [2].
Concurrently, chronic noise exposure can cause progressive degradation of the peripheral vestibular system [11]. Saccular and utricular hair cells, which are sensitive to low-frequency acoustic vibrations, can undergo structural damage under continuous acoustic overstimulation [11].
This damage is marked by a loss of calretinin-positive calyces within the striolar region of the vestibular otolith organs [12]. Electrophysiologically, this degradation manifests as prolonged latencies and reduced wave amplitudes in cervical vestibular evoked myogenic potentials (cVEMP) and vestibular short-latency evoked potentials (VsEP) [12] Clinically, this vestibular loss presents as balance deficits, spatial disorientation, unsteadiness, and vertigo, significantly elevating the risk of falls [12].
Irritant Reactions: Tonic Tensor Tympani Syndrome and Sterile Inflammation
At the mid-level of the pathological hierarchy, intense or sudden acoustic parameters generate direct physiological irritation within the auditory and somatic nervous systems [1]. This sensory irritation is driven by two key pathways: neuropathic muscle spasms and cellular sterile inflammation [35].

At the neuropathic level, sudden, unexpected, and high-pitched acoustic events (such as feedback screeches, alarms, or public address system squeals) trigger Acoustic Shock ().35 The physiological basis of AS is Tonic Tensor Tympani Syndrome ().38 The tensor tympani is a middle ear muscle innervated by the mandibular branch of the trigeminal nerve ().23 Under normal conditions, it contracts to support the ossicular chain.23
However, under high psychological stress or during an unexpected acoustic incident, the threshold for this reflex is reduced, causing persistent, involuntary contractions and muscle spasms.23
These chronic muscle spasms cause physical tension on the tympanic membrane, altering middle ear ventilation and causing a sensation of ear blockage, pressure, and tympanic flutter.35
Furthermore, the hyper-contraction of the tensor tympani directly irritates and inflames the trigeminal nerve endings.35 This irritation triggers severe neuropathic ear pain, often described as a sharp, stabbing sensation resembling an electric shock, alongside localized burning, numbness, and tingling around the ear, cheek, jaw, and neck.35
At the cellular level, intense noise overexposure damages the cochlea, which triggers a sterile inflammatory response.36 Tearing of the organ of Corti and damage to the sensory hair cells releases intracellular molecules that act as damage-associated molecular patterns ().9 These DAMPs bind to innate immune receptors (such as Toll-like and NOD-like receptors) on surrounding supporting cells and fibrocytes, activating inflammatory cell stress pathways.36
This pathway drives the transcription and release of pro-inflammatory cytokines, specifically tumor necrosis factor-alpha () and interleukin-1 beta (), as well as chemokines like CCL2.36 These chemical signals recruit circulating monocytes and pro-inflammatory macrophages into the scala tympani, spiral ligament, and lateral wall.36 This inflammatory cascade can cause further hair cell death and accelerate progressive sensorineural hearing loss.36
Infectious Diseases: Tympanic Perforation, Eustachian Dysfunction, and Secondary Otitis
When acoustic parameters reach extreme physical energy levels—such as blast overpressures or high-intensity impulse noise exceeding SPL—the human ear is subjected to severe structural trauma.8
At these decibel levels, the mechanical force of the pressure wave exceeds the tissue elasticity of the middle ear.9 This force causes physical tearing, resulting in tympanic membrane perforation, and can fracture or dislocate the middle ear ossicular chain (the malleus, incus, and stapes).8
This mechanical trauma removes the primary physical and immunological barrier of the middle ear.9 Normally, an intact tympanic membrane isolates the mucosal middle ear cavity, maintaining a sterile environment.9
Once this barrier is ruptured, the sterile middle ear space is directly exposed to external biological contaminants, including opportunistic bacteria (such as Streptococcus pneumoniae and Pseudomonas aeruginosa) and fungi.1
This microbial invasion can lead to acute otitis media (middle ear infection), presenting with severe earache, fever, throbbing pressure, and purulent fluid discharge.47
If middle ear ventilation is also compromised by concurrent Eustachian tube dysfunction (which is common following structural ear trauma), the infection can become chronic.23 The inflammatory process can then spread into the surrounding temporal bone, causing:
Acute Mastoiditis: The infection spreads into the mastoid air cells, causing severe retroauricular pain, redness, swelling, bone destruction, and high fever.47
Labyrinthitis (Inner Ear Infection): Pathogens or toxic inflammatory byproducts pass through the round or oval windows, directly infecting the fluid-filled cavities of the cochlea and vestibular apparatus.46 This causes severe inner ear inflammation, presenting with vertigo, loss of balance, nausea, vomiting, and permanent sensorineural hearing loss.46
Toxic Chronic Effects: Apoptosis, eNOS Uncoupling, and Arterial Remodeling
At the level of chronic effects, long-term exposure to acoustic parameters generates permanent, irreversible damage to both the auditory cells and the vascular system [1].
In the auditory system, chronic noise overexposure () causes progressive sensorineural hearing loss () [9]. This toxic chronic effect is driven by metabolic exhaustion within the cochlea.9 The continuous energy load drives mitochondria to overproduce reactive oxygen and nitrogen species (/), causing chronic oxidative stress [10].
This oxidative stress damages intracellular proteins, lipids, and DNA, activating caspase-dependent and caspase-independent apoptotic pathways.20 This results in the death of outer hair cells in the basal turn of the cochlea, leading to a permanent reduction in hearing sensitivity centered around the frequency [9].
In the cardiovascular system, chronic exposure to environmental noise () drives vascular remodeling through systemic oxidative stress and endothelial dysfunction [2].
The chronic, sub-cognitive activation of the axis and stimulates vascular NADPH oxidase, causing the overproduction of superoxide anions () in vascular tissue [13]. These superoxide radicals react with vascular nitric oxide (), forming peroxynitrite () and reducing bioavailability [2].
Peroxynitrite then oxidizes tetrahydrobiopterin (), an essential cofactor for endothelial nitric oxide synthase () [2]. Deprived of , eNOS undergoes uncoupling, shifting from producing vasodilatory nitric oxide to generating superoxide radicals, which further amplifies vascular oxidative stress [2].
This state of uncoupled eNOS and chronic vascular oxidative stress promotes:
● Vascular Inflammation: Upregulates adhesion molecules like VCAM-1, recruiting pro-inflammatory macrophages into the vascular intima.50
● Atherosclerosis: Accelerates the oxidation of low-density lipoproteins () and the formation of foam cells, leading to plaque accumulation in the coronary and cerebral arteries [13].
● Systemic Arterial Hypertension: Chronic vasoconstriction and vascular remodeling permanently raise peripheral vascular resistance [2].
Cardiovascular Mortality and Critical Exposure Thresholds
The terminal endpoint of the acoustic pathological hierarchy is cardiovascular mortality.2 Chronic exposure to transportation and environmental noise acts as an independent risk factor for major adverse cardiovascular events (), including fatal myocardial infarction (heart attack) and ischemic stroke [2].
Epidemiological Burden and Exposure-Response Relationships
Epidemiological and public health data demonstrate a clear relationship between environmental noise exposure and cardiovascular mortality [2]. According to the European Environment Agency () 2025 report, chronic transportation noise exposure contributes to:
● Premature Deaths: At least premature deaths annually in Europe.4
● Ischemic Heart Disease: Approximately new cases of ischemic heart disease () annually [4].
● Type 2 Diabetes: At least newly attributed cases of type 2 diabetes annually, driven by chronic cortisol-induced insulin resistance [4].
● Total Disease Burden: Over disability-adjusted life years () lost annually in Europe due to environmental noise [54].
The World Health Organization () Environmental Noise Guidelines establish specific exposure-response thresholds where the risk of cardiometabolic disease increases significantly 2:
● Road Traffic Noise: Risk of ischemic heart disease () increases by for every increase in starting at an exposure threshold of [58]
● Overall Transport Noise: A combined meta-analysis demonstrates that for every increase in , the risk of developing heart attack, stroke, or heart failure rises by [5].
● Nocturnal Noise: To prevent sleep fragmentation and vascular damage, the WHO recommends that nocturnal noise exposure () from road traffic does not exceed [2].
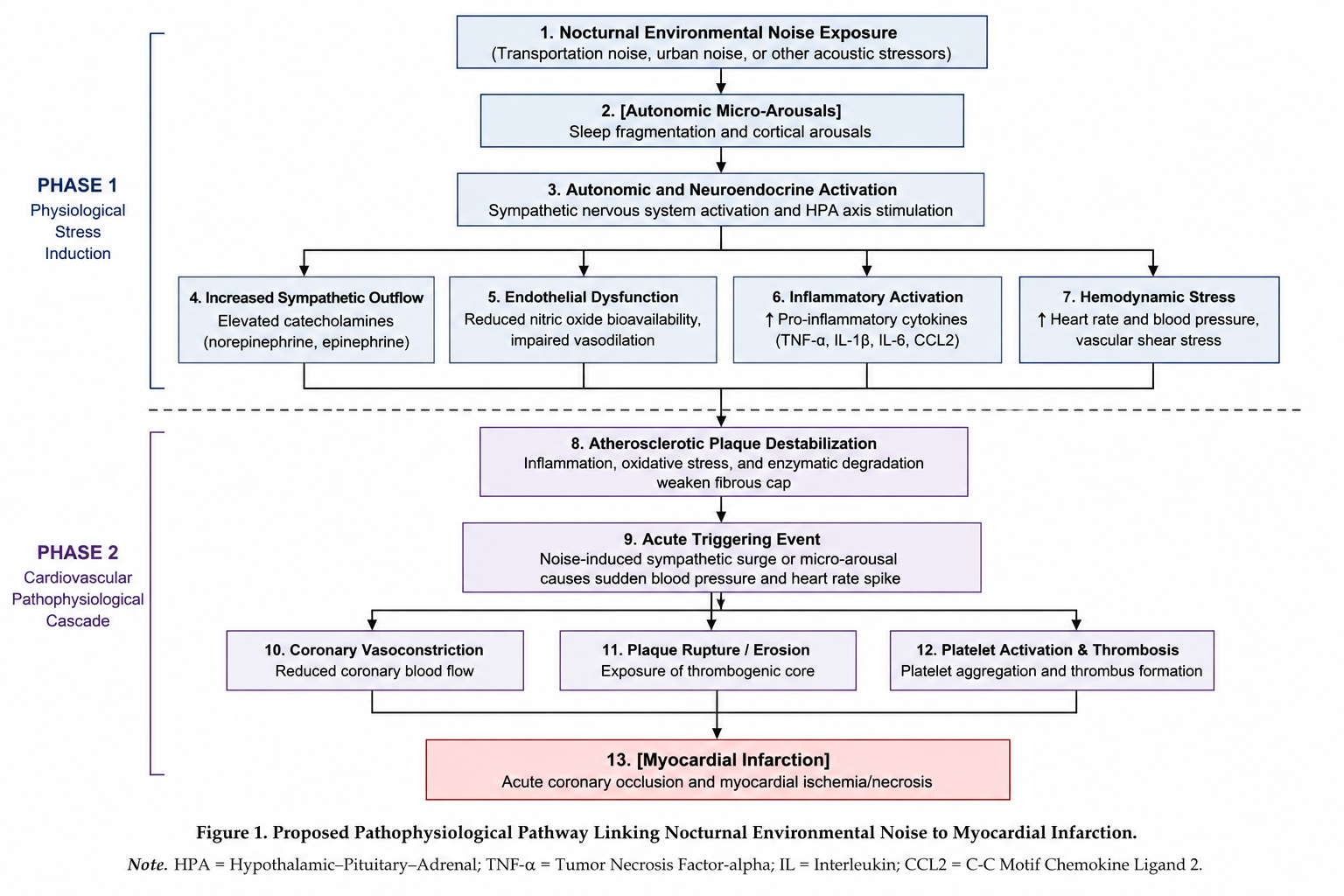
Acute Triggering of Fatal Events
In addition to driving chronic vascular damage, environmental noise can trigger acute, fatal cardiovascular events [2]. In patients with pre-existing atherosclerosis, a sudden, loud nocturnal noise event or persistent sleep disruption can trigger a massive surge of catecholamines [2]. This spike in epinephrine causes a rapid increase in blood pressure, heart rate, and coronary vasoconstriction [28]. The resulting mechanical shear stress can rupture unstable plaques in the coronary arteries [52].
Plaque rupture triggers rapid platelet aggregation and thrombosis, completely blocking coronary blood flow and causing a fatal acute myocardial infarction [2].
Furthermore, sudden, intense emotional or physical acoustic stress can trigger Takotsubo cardiomyopathy stress-induced cardiomyopathy or neurogenic stunning of the heart [30]. This condition is driven by a profound surge of catecholamines that stuns the myocardium, presenting with severe chest pain, acute left ventricular dysfunction, heart failure, and fatal ventricular arrhythmias [30].
Noise Control as Preventative Strategies
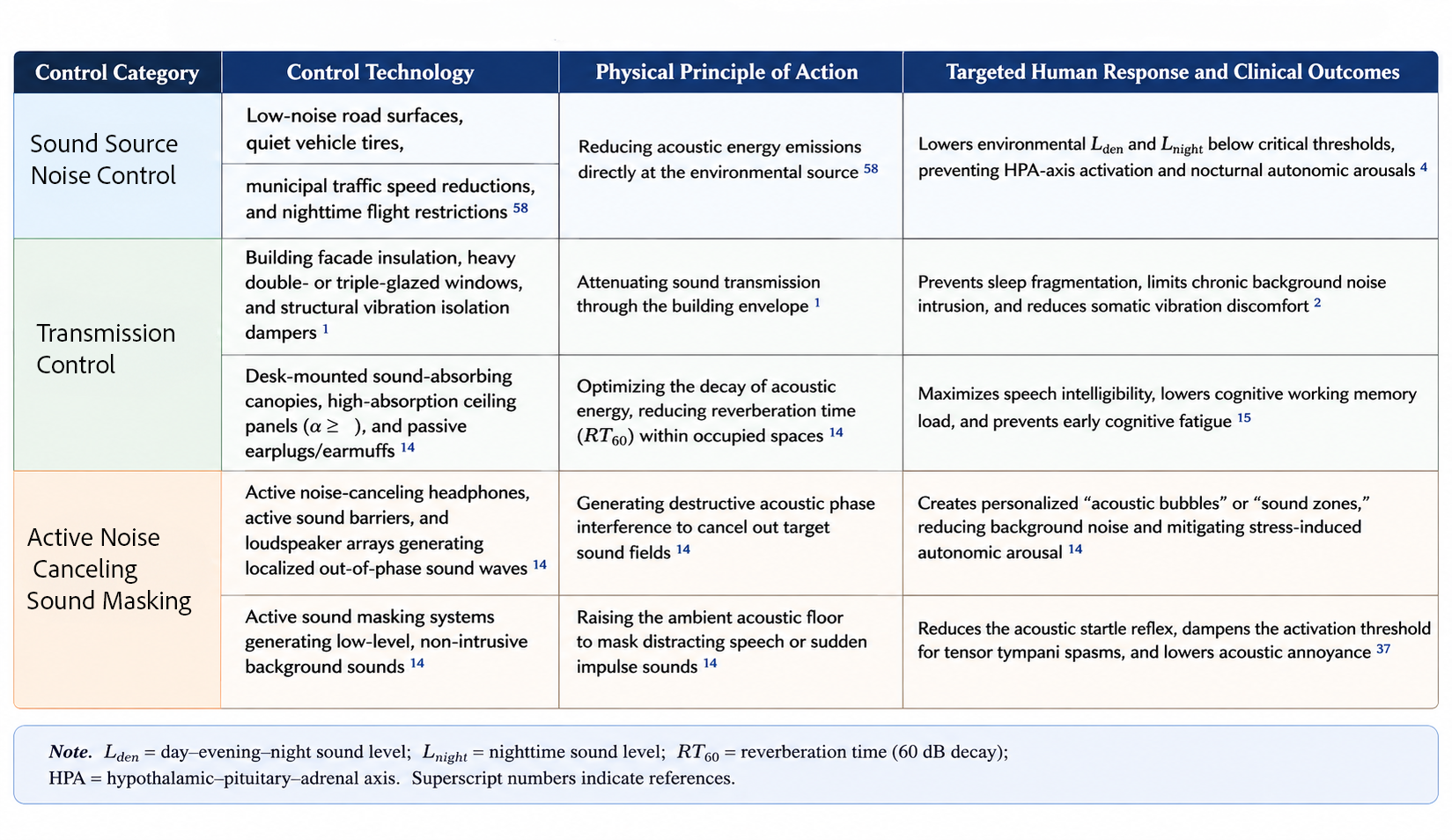
Mitigating the physiological effects of acoustic parameters requires combining source-level noise control with occupant-centric building design [1]. These approaches are categorized into acoustical control, passive noise control, and active noise control [6].

Sound Source Control
The primary line of defense is acoustical control at the source, which aims to reduce noise emissions before they enter the human environment [58]. At the municipal level, this includes implementing low-noise asphalt road surfaces, regulating quiet vehicle tires, establishing urban speed limits, and restricting nighttime flights over residential areas [58]. Controlling these parameters helps keep residential exposure levels below the and targets required to protect long-term cardiovascular health [4]
Noise Insulation - Barrier Control
Passive noise control focuses on architectural path attenuation.14 This includes increasing the sound insulation of the building envelope using heavy, double- or triple-glazed windows, and placing structural vibration isolation dampers under mechanical equipment.1 Internally, passive control involves installing sound-absorbing ceiling panels to reduce the reverberation time () [17].
Personal Sound Control - Hearing Protection
Additionally, passive Acoustic Personalized Environmental Control Systems ()—such as desk-mounted sound-absorbing canopies, passive earplugs, or earmuffs—can be used to reduce localized sound levels.14 These passive systems lower background noise, improve speech intelligibility, and reduce the cognitive load on occupants [18].
Active Noise Control - Sound Masking
Active noise control utilizes electronic systems to generate out-of-phase sound waves that cancel out target sound fields.14 This is implemented through active noise-canceling () headphones, earbuds, or active localized loudspeaker arrays that create sound-masking zones in open-plan offices [14].
These systems are highly effective at neutralizing low-frequency noise (), which is difficult to block with passive architectural barriers.11 Active noise control helps lower the acoustic startle reflex, prevents involuntary middle ear muscle spasms, and dampens systemic autonomic stress responses [14].
Conclusions
Acoustic parameters operate on a continuous pathological spectrum that directly affects human health [1]. While elevated background noise and prolonged reverberation times cause localized discomfort, speech interference, and early cognitive fatigue, chronic exposure to low-to-moderate environmental noise 50 dBA - 60 dBA triggers systemic stress pathways [2]. This chronic neuroendocrine activation drives arterial hypertension, endothelial dysfunction, eNOS uncoupling, and progressive vascular remodeling, significantly elevating the risk of cardiovascular mortality [2]. At higher physical intensities, sudden acoustic events cause acute neuropathic irritation (Acoustic Shock and Tonic Tensor Tympani Syndrome) or structural middle ear trauma, which predisposes the ear to secondary pathogenic infections like acute otitis media and labyrinthitis [8].
Protecting human health requires moving beyond traditional regulatory frameworks that only address direct hearing loss.1 Modern public health policy and architectural engineering must treat environmental and transport noise as a major modifiable cardiovascular and metabolic risk factor [4]. Facade insulation, localized sound absorption, and active noise control are critical to keeping cumulative exposures below WHO guidelines [4].
Furthermore, integrating acoustic control with indoor air quality management is essential [1]. This dual approach prevents the mucosal congestion and Eustachian tube inflammation that can compromise middle ear mechanics and exacerbate acoustic stress [1]. Ultimately, environmental noise mitigation must be treated as a central pillar of preventative medicine and sustainable urban design to reduce the global burden of cardiometabolic disease and prevent premature mortality [4].
References
1. Understand Indoor Envrionment Quality.pdf
2. Transportation Noise Pollution and Cardiovascular Health | Circulation Research
3. Noise and air pollution as risk factors for hypertension: part II – pathophysiologic insight
4. New EEA 2025 Noise Report Confirms: Environmental Noise is a Medical Emergency
5. Traffic noise, a novel risk factor for cardiovascular diseases
6. uploaded:Screenshot 2026-05-27 at 11.29.44.png-48e61f47-4bbc-4654-96f6-e15406f0f270
7. How different sounds affect bodily responses and the perception of odour, light and temperature - Taylor & Francis
8. Acute Acoustic Trauma: Symptoms, Causes, and Treatments - Audibel
9. Previous Chapter: Case Study 52: Behavioral and Audiologic Manifestations of Noise-Induced Hearing Loss - National Academies of Sciences, Engineering, and Medicine
10. Acute Acoustic Trauma - StatPearls - NCBI Bookshelf
11. Noise-induced vestibular dysfunction in rats: longitudinal assessment using cVEMP and behavioral testing after low-frequency acoustic trauma - PMC
12. David S. Bauer's research works | University of Michigan and other places - ResearchGate,
13. Environmental Noise and the Cardiovascular System - PubMed,
14. (PDF) Introducing the concept of Acoustic Personalised Environmental Control systems (Acoustic PECS) within the framework of IEA EBC Annex 87 - ResearchGate,
15. Life Cycle Value Tradeoff of Noise Mitigating Measures Using BIM-Simulation and Multi-Criteria Decision Modeling - IFMA Knowledge Library,
16. Transportation Noise and Cardiovascular Health: Evidence, Mechanisms, and Policy Imperatives The Anatolian Journal of Cardiology,
17. Effects of Classroom Acoustics and Self-Reported Noise Exposure on Teachers' Well-Being,
18. Effects of reverberation time on the cognitive load in speech communication: Theoretical considerations | Request PDF - ResearchGate,
19. The effects of classroom acoustic quality on student perception and wellbeing: a systematic review across educational levels - PMC,
20. Noise reaction scheme explaining the adverse cardiovascular effects of... - ResearchGate, accessed May 27, 2026.
21. Noise annoyance and cardiovascular disease risk: results from a 10-year follow-up study, accessed May 27, 2026.
22. Improving indoor air quality and aesthetics in an economical and environment-friendly way by utilizing decorative indoor plants - ResearchGate
23. Tonic tensor tympani syndrome - Wikipedia
24. Vestibular Findings Associated with Chronic Noise Induced Hearing Impairment
25. Tensor Tympani Syndrome - StatPearls - NCBI Bookshelf - NIH
26. Influence of Classroom Acoustics on Noise Disturbance and Well-Being for First Graders
27. [PDF] The Indoor Environment Handbook by Philomena Bluyssen | 9781136544811 - Perlego
28. Heart Problems: Scary Stress Responses Known - Liv Hospital, accessed May 27, 2026
29. Understanding the stress response - Harvard Health
30. The effects of stress on the heart | Prevention Observatory of the Montreal Heart Institute
31. Chronic stress puts your health at risk - Mayo Clinic
32. Noise-induced Vestibular Dysfunction: An Unexplored Entity | Request PDF - ResearchGate
33. The effect of noise exposure on vestibular function - White Rose eTheses Online,
34. Association between Simultaneous Occurrence of Occupational Noise-Induced Hearing Loss and Noise-Induced Vestibular Dysfunction: A Systematic Review - PMC
35. Acoustic Shock and Tensor Tympani Syndrome (TTS) - DWM Audiolog
36. Inflammation associated with noise-induced hearing loss - PMC - NIH,
37. Acoustic Shock - The Royal Victorian Eye and Ear Hospital
38. Tonic tensor tympani syndrome in tinnitus and hyperacusis patients: A multi-clinic prevalence study - Macquarie University
39. Tonic tensor tympani syndrome in tinnitus and hyperacusis patients: a multi-clinic prevalence study - PubMed,
40. Acoustic Shock Disorder | The Hyperacusis Network
41. A Beginner's Guide To Tensor Tympani Syndrome - Treble Health, accessed May 27, 2026
42. Tonic Tensor Tympani Syndrome - AVI New England
43. Acoustic Shock | Canadian Audiologist,
44. Acoustic Trauma: Signs of Long-Term Risks and Ear Ache | The Harley Street ENT Clinic
45. Tensor Tympani Syndrome (TTS) - DWM Audiology
46. Inner Ear Trauma | Suarez Physical Therapy,
47. Ear Problems: Causes, Symptoms & Treatment Options - The MED-EL Blog
48. Adenosine and the Auditory System - PMC
49. The relationship between noise pollution and cardiovascular diseases: an umbrella review on meta-analyses - PMC
50. An underestimated danger: Noise and air pollution are new and important cardiovascular risk factors
51. Long-Term Effects of Aircraft Noise Exposure on Vascular Oxidative Stress, Endothelial Function and Blood Pressure: No Evidence for Adaptation or Tolerance Development - Frontiers
52. Yes, Stress Can Hurt Your Heart: 3 Things to Know | News - Yale Medicine,
53. Circulation Research, https://www.pleanala.ie/publicaccess/314485%20-%20Case%20Documentation/314485/Responses/Responses%20&%20Submissions%20to%20Draft%20Order/Liam%20O'Gradaigh%2023.12/Liam%20O'Gradaigh%20Part%204%2023.12.pdf
54. Transportation noise pollution as a cardiovascular risk factor: from epidemiological evidence to mechanistic insights - PMC
55. Longevity and Environmental Perception: Introducing Life Years Without Pollution or Noise Across Europe - EPC2026
56. Environmental noise in Europe - 2025
57. Revisiting the association between transportation noise and heart disease reported in the World Health Organization Environmental Noise Guidelines for the European Region: a systematic review and meta-analysis - PubMed,
58. Effects of noise exposure on the cardiovascular system. - Medizinonline
59. Environmental Impacts on Cardiovascular Health and Biology: An Overview - PMC - NIH,
60. Noise | In-depth topics | European Environment Agency (EEA)
61. Optimum acoustic conditions for a speaker as a function of the... | Download Scientific Diagram - ResearchGate